


£50k pa jobs for people currently on benefit? What’s the business model? #Employment
The 3 Es: Employment, ‘Ealth and Education



Photo by Damien TUPINIER on Unsplash
If the New Deal kick-started the US economy using largely manual jobs the next big wave of job creation may be around skills and knowledge. This series is exploring the challenge of creating hundreds of thousands, perhaps a few million, new jobs with salaries north of £50k p.a.
Success at this level would certainly transform the the UK economy and if those landing such new jobs were previously in receipt of benefit, there would be a double whammy.
Is it possible?
In the previous post we looked at a couple of communities that possess unusual skills and yet are unable to monetise them. We looked at carers who have learned how to navigate the NHS and yet all their skills are expended for free in supporting a single person’s care journeys. Worse still, many of them would have given up work to become a carer!
Is there a way to focus such knowledge into a valuable navigation service and are there clients for such a service? Is there is a clear value proposition? We believe the answers are yes, but they are not easy.
Let’s turn to the easier example from the previous post of building a business in medical device assessment using people who use assistive and other medical technology every day. The MedTech sector is worth more than €500billion p.a. and the usability of every product must be established, increasingly for regulatory reasons. There should also be a commercial premium associated with more useable technology, and ensuring user engagement at the right points in product development cycle is a critical challenge and one where Prof Young led a 10-year research programme.
A team of experts offering formal assessment with an innovation wrap-around to enhance usability with a combination of health economic, regulatory and business case support, could really help MedTech manufacturers and vendors but also healthcare providers as smart customers purchsing such technology.
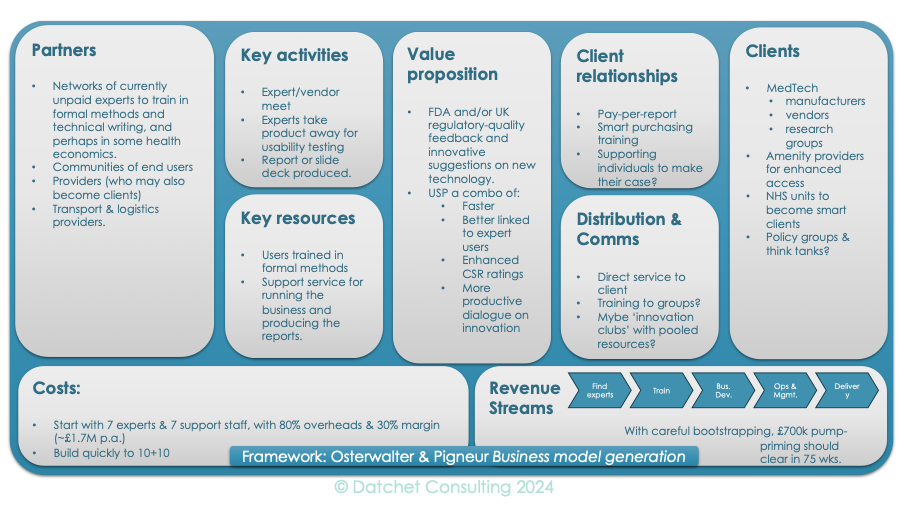
Expert testing: the visuals
This feasibility overview is based on Business Model Generation by Osterwalder and Pigneur, and which is available physically and as an e-book. Their visualisation proposal is a single diagram with several boxes that address the big issues and can be filled in with words or drawings, which Datchet Consulting and The Young Analyst have filled in.
For anything to do with projects or planning, you always start at the end. Essentially you imagine where you want to get to and then work backwards to where you are now, and the path forward should light up before you.
There are three main clients in view, with a smaller but potentially higher-value community on the edge. Mainstream clients are MedTech vendors. This space will have changed, perhaps radically, since Prof Young was researching it, but from the lack of success in making new and better technology stick in the NHS, it looks like we aren’t that far away. At one level, there is plenty of support for MedTech – for free and for fee – but much of it is disconnected.
Two seminal experiences come back from that period. One was a piece of consultancy undertaken for part of the NHS many years ago that was looking for technology to cut the NHS spend by £5billion a year. Clearly, big companies with their teams of health economists should the best cases but the surprise was how many ignored basic costs of introduction, such as who would use it and how. If a new widget takes three steps out of conventional patient pathways, what does the new pathway look like? Who will specify the new steps of care? What happens to the staff delivering conventional care – do they carry on or are they replaced and if so, what does the phasing look like? These questions are all about users; they are all expensive and they were all cheerfully ignored in many submissions.
The other vivid memory was a trip to California, where the British Embassy had set us visits to MedTech start-ups. These entrepreneurs had met everyone from the Secretary of State for Health on down but had no clue as to how to build an evidence base that NICE, for example, would accept. In setting up these (free) networking opportunities for the industry, FCO was behaving as though it was short of money but had plenty of time. The reverse was true: these start-up could burn hundreds of thousands of dollars a month, but were chronically short of time.
MedTech is therefore a potential client group, but it will probably take a pincer movement before radically better technology hits the market at more realistically affordable prices – customers need more of a voice. The NHS has been labelled as a poor adopter for decades, but that’s an easy accusation that’s hard to counter. What is really needed is timely, accurate, well-scored information on what works best for patients to differentiate it against what is theoretically effective but will pile up the spare bedroom.
Both these groups have a sense of need and may lack an effective sense of urgency but the guts of a market lies in stitching their needs together, and those with impairment are much more intuitively aligned to the problems that those who ask them questions and report on their behalf.
Clearly, someone advises hotels and the like about meeting disability legislation with accessibility and special facilities, but the variation is extreme. I’ve been in motorways service stations that had tens of thousands of pounds of smart loos and powered changing platforms, and in high end retreats where the disable changing room was essentially unusable (and full of junk). There must be a market there for those with lived experience and mastery of formal methods to add hundreds of thousands of pounds of value a month to our amenities and leisure industry.
Without working through every box, it should be clear that we envisage a service industry where experts with their own experience of impairment take on usability projects for research, regulatory reporting or to drive better marketing. Since mobility will be a problem for many, why not add a luxury branding with chauffeur driven-arrival for briefings or collecting prototypes? Reports, live presentations, or videos could provide feedback to the board, while in-depth discussions with technical staff would drive innovation and adoption.
Where would the expert staff come from? A friend of mine who works in rehabilitation notes how many people who present have Masters degrees and no jobs. That’s where I’d start. People who study for their own pleasure clearly have the neurons and most of are highly IT literate. Some training is a natural next step to enable them to turn a lifetime of mixed experiences, missed appointment and disappointing solutions into rewarded, well remunerated, work.
A team of 7 experts supported by a team of 7 administrators and managers, finding more experts, developing business, writing copy, filming and producing artwork, might burn £100k a month until it started gaining traction. How much risk the workforce might share would be up for grabs, but once operating, this could be a gold-mine!
Any takers?
 | A guest post by
|