
Dear Mr Streeting, mind the STEPS!
An occasional letter


Dear Secretary of State for Health and Social Care,
In a bound you are free of a layer of infrastructure costing £3Bn p.a., I hear. That’s the easy bit! The hard part is delivering with or without it.
I’m taking a break this Thursday from releasing chapters of my book about health management – Dark Matter – to reflect on where next. The chapters from Dark Matter already posted are listed at the bottom.
This piece is short, so I’ve listed 7 posts on Fixing the NHS at the end, with suggestions about the trip hazards I describe.
The STEPS
To avoid being swallowed up by whatever engulfed NHS England, there are 5 STEPS you may want to watch out for. I don’t think NHS England really got them, and in the end, they got NHS England.
Scale. There is no ideal unit size, only trade-offs around wherever you start
Technology really matters but the NHS’ record is tragically mixed
Employment is key, so you’ll need solutions that deliver jobs with wellness
Plans. You’ll need to do better than NHS England did. Better plans are available
Systems are slick as soap – NHS England slipped on the dangers instead of grasping the potential
My pitch for a hearing is threefold.
Ever since the Six Day War, when we were airlifted out of Beirut and I ended up at Roehampton, I’ve used NHS limbs and other services. For almost 60 years, I’ve seen some of the best and poorest aspects of the service from the inside.
With a STEM first degree and PhD, I understand systems.
For nearly 30 years, my research (industrial and academic) lay in UK care delivery, and also in Australia, the US and parts of Europe.
The tekkie-patient combo is relatively unusual. Add a quarter of a century in leading research, and there are not many of me about. It hasn’t made me smart enough to solve it all, but it’s yielded rare insights into why so much has failed this century.
Scale
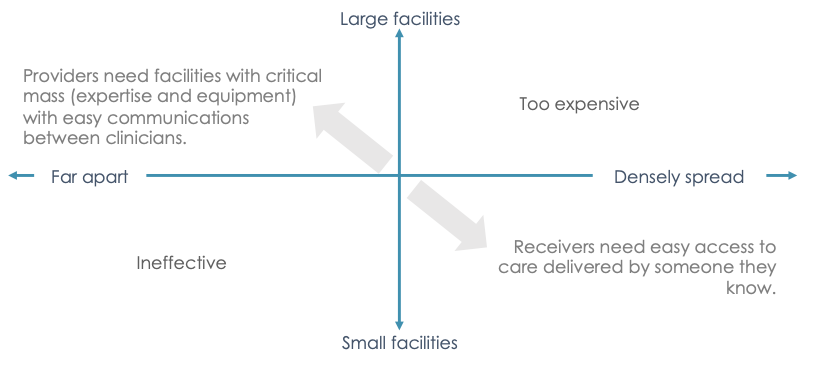
This chart shows that providers like to cluster services into dense hotspots of people who know their stuff. Users prefer stretched-out services, hoping to find someone nearby who knows their name.
NHS England reflected this paradox in that clustering knowledge and decision-making into a single hotspot left too many bases uncovered.
When I left Marconi and became a professor at Brunel, the late Peter Craine (Head of Government Affairs at Marconi) got me an appointment with Paul Corrigan, who was Alan Milburn’s advisor. I duly arrived at Richmond House with a pitch for transforming the NHS. Paul’s objection – and hindsight proved him correct – was that the NHS wasn’t a single organisation. There was nowhere to stand with your lever if you wanted to move the earth.
Scale is weird, and cracking scale not simply about removing layers or disaggregating into smaller units any more than it was ever about integrating into larger Trusts or even ICS’s.
Technology
While logistics, materials, miniaturisation and scanners matter, health is a knowledge industry and so ITC (Information Technology & Comms) is king.
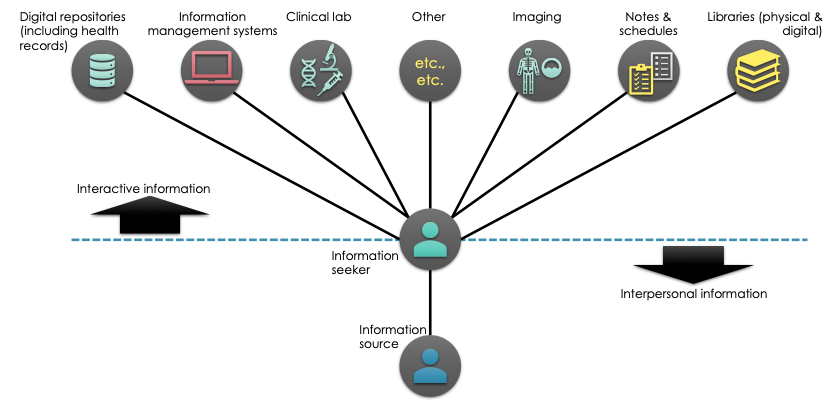
This chart shows that for care delivery to work, everyone – from patients to Secretaries of State – must have rapid access to knowledge. This comes from all over the place but only in two flavours – information (above the line) and dialogue (below).
Above the line, the NHS (most health services, to be fair) is patchy and below it, things haven’t moved much for patients since the Penny Black and Alexander Graham Bell. Everything new, especially apps, is targeted above the line, so that timely dialogue is frequently impossible.
Technology has boosted quality and slashed costs everywhere except in health, where this century has been a guide mainly in how not to. Please don’t trip over the technology!
Employment

Photo by ThisisEngineering on Unsplash
The NHS hasn’t worried much about whether people are working or not, so it’s become a bit of a time bandit, stealing hours and days from job holders through appointments and faff.
Along with education, health sees disability as a problem to be fixed, which is what let the time bandits loose in the first place. Without fierce resistance, you become a mission for the system and lose your life to being fixed.
I like to think that disability often has an upside; not a superpower, but something striking and unusual. If you can tap into that – especially with neurodiversity and some of the mental health issues that have been exercising you recently – you may switch people from benefits (which is where they end up once they are being fixed) into high earning taxpayers. It won’t be easy, but I don’t think it’s really been tried, yet.
If you can step up to this, your problems will recede because working folk are healthier and they channel cash into the exchequer.
Plans
NHS England was always planning and demanding plans. You’ll need a plan that delivers:
Hope, with tangible improvements in 1 year and widespread reform in 5
Using ITC, logistics, scanning, etc, properly to slash costs for better outcomes
At modest up-front cost that yields year-on-year savings after that
Through a domino cycle of savings and better quality that liberates more savings and better quality, until it percolates throughout the service
It’s nigh on impossible, but maybe not quite.
Systems
The big idea this century has been systems, with information transformation in the early noughties and latterly with ICS’s.
While systems have amazing upsides, they have a deadly downside and it’s this. When you intervene, they push back strongly towards what they were doing before, so interventions that target specific problems get swamped by the system’s recovery reaction. This means you need something remarkable and wide-ranging, or change will take a terrible toll.
So far, we’ve seen a bit of the latter. Your mission is to facilitate the former.
All the best!
Suggestions
Fixing the NHS: hurdling todays barriers for a fitter future (25 July 2024)
Fixing the NHS: the digital arts and a simple knowledge model (1 August 2024)
Fixing the NHS: the digital arts and service design (8 August 2024)
Fixing the NHS: the digital arts and getting the right numbers (15 August 2024)
Fixing the NHS: making the virtuous vortex work (22 August 2024)
How to design a centre that closes 4,000 patient journeys a month for £1,000/patient or less, all in (29 August 2024)
Fixing the NHS: the bite-sized story in 6 charts (5 September 2024)
Dark Matter: vital invisible management skills
Intro and chapters 1-6 released so far
Health Management: is there a problem? [Dark Matter introduction](30 January 2025)
The Dark Matter of saving time in health management [Dark Matter chapter 1] (6 February 2025)
The Dark Matter of creating time in health management [Dark Matter chapter 2] (13 February 2025)
The Dark Matter of small teams in healthcare [Dark Matter chapter 3] (20 February 2025)
The Dark Matter of team players in healthcare [Dark Matter chapter 4] (27 February 2025]
The Dark compulsions of counting in healthcare management [Dark Matter chapter 6] (6 March 2025)
The Dark Matter of simply managing in health [Dark Matter chapter 5] (13 March 2025)